 NV.gov
NV.gov
Zika Virus
Zika Virus In Nevada's Communities
As of January 25, 2017 Nevada has 19 reported cases of travel-associated Zika Virus Cases. Nevada does not have any locally acquired cases.
To get up to date state-by-state Zika related information and maps, please visit the CDC's website
CDC Zika Updates (click image below to access CDC's site)
Zika Virus - Information about the Virus & Current Updates
") Zika Prezi Presentation (click map to access)
Zika Prezi Presentation (click map to access)
Accompanying guidance to CDC Guidelines for Development of State and Local Risk-based Zika Action Plans *Does not include guidance specific to US territories
Early season mosquito control efforts can decrease the risk of eventual Zika transmission. In addition, effective control of Zika will depend on prompt and aggressive intervention when human cases are first identified. All at-risk communities should prepare for Zika virus activity, and should evaluate and prepare control plans for mosquito populations in their state as part of Zika Action Plan preparedness efforts. A comprehensive review of health code, enforcement practices and property access will aid the implementation of a vector control plan.
Many states already have vector control programs. With the exception of states who have responded to past outbreaks of dengue and chikungunya, most state plans focus on control of mosquitoes for the prevention of West Nile virus (WNV). The biology and behavior of Aedes aegypti and Aedes albopictusare different from the mosquitoes that transmit WNV. Therefore, the tools used for surveillance of these species as well as strategies for control will be different from WNV mosquitoes.
Before mosquito season
- State, tribes, and local governments should consider using an Integrated Vector Management (IVM) strategy as they develop their mosquito control plans (See Appendix).
- Public health officials and vector control officials should develop a communications network to ensure timely exchange of information, and collaboratively share information to guide optimum vector control efforts. This network should be part of the state’s Incident Management structure, and should report efforts and plans to the state Incident Manager (IM).
- To prepare for the possible introduction of Zika virus, states, tribes, and local governments should review historical data and maps regarding the presence of Aedes aegypti and Aedes albopictus. If maps are outdated and resources permit, plan new surveys and assessments to be conducted during mosquito season.
- Responding officials should review existing staffing capacity, resource allocation, and technical expertise at the local level for vector control and consider use of intergovernmental agreements for vector control to help adjacent counties outside their jurisdiction, as well as pre-positioning contracts with vendors to supply additional capacity.
- Responding officials should link vector control efforts with communication efforts. This includes ensuring public education campaigns include information not just on personal protection measures, but also how citizens may reduce or eliminate breeding sites for Ae. aegypti and Ae. albopictus, and to motivate the community to remove and dispose of any water holding containers
Mosquito season
- Using the plan previously developed, survey and map presence of Aedes aegypti and Aedes albopictus within the state.
- Actively engage community to encourage removal of larval habitat and Aedes breeding sites, including community cleanup campaigns (tire removal, trash pickup, removal and cleaning of small and large containers). Leverage partnerships with local governments and non-profits for support.
- If resources and technical expertise permits, conduct rapid insecticide resistance testing for local mosquito populations, in order to know the pesticides most likely to be effective in the event of Zika transmission.
- Use larvicides in containers and bodies of water that cannot be removed or dumped.
Confirmed transmission (first case, or several cases in a single household or building)
- mplement Targeted Control efforts around the case-patient’s home or building. Conduct intensified larval and adult mosquito control in a 150 yard radius (or other boundary as deemed appropriate) around the case patient home. Targeted control activities involving home visits should be closely coordinated with concurrent educational efforts and messaging.
- Consider adding community-based adult mosquito control consisting of outdoor residual spraying, and space spraying if necessary.
- Intensify larviciding and source reduction efforts.
- Consider targeted indoor residual spraying in areas where A/C and screens aren’t widely available.
Widespread transmission within a county or jurisdiction
- Vector control efforts should align with state, tribal, and local government decisions regarding boundaries for declaring an area as a site of “active Zika transmission”. This may model county lines, or be a zipcode designation. At this phase, officials should plan to intensify and expand vector control efforts within the areas of active transmission.
- In addition to continuing to target case-patient homes and the surrounding vicinity, area-wide treatments with larvicides and adulticides using application methods appropriate for the scale of the treatment area should be considered. Control plans should be tailored to the local needs, and might require truck or aerial spraying (aerial for areas > 2,000 acres) or a combination of both.
- Monitor for effectiveness of treatments through trapping and retreat if mosquito numbers begin to increase again.
- For areas where A/C and screens aren’t widely available, consider adding targeted indoor residual spraying to vulnerable homes.
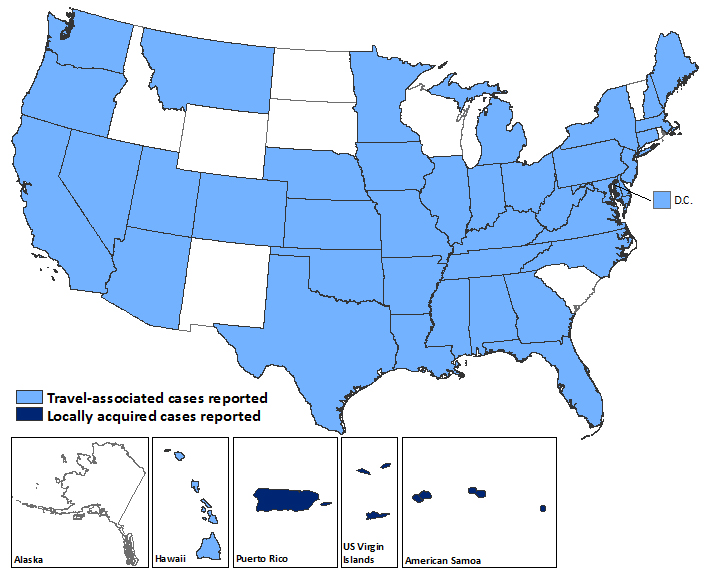 This image may not be the most current information available. Please click on the map for the most up to date version
This image may not be the most current information available. Please click on the map for the most up to date version